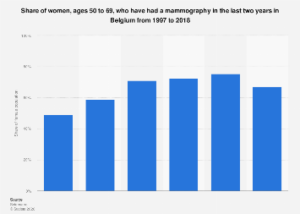

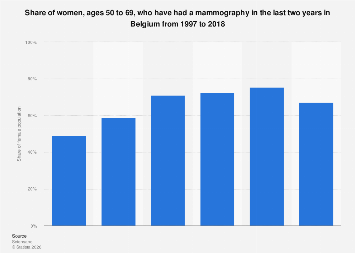
In 2018, a significant two-thirds of Belgian women aged 50 to 69 had undergone mammography screening, a critical tool in the early detection of breast cancer. This figure, while substantial, marked a slight decrease from previous years, indicating a nuanced evolution in screening participation within this age demographic. Analysis of data spanning from 1997 to 2018 reveals a generally upward trajectory in the proportion of women in this age group availing themselves of mammograms, underscoring a growing awareness and adoption of preventative health measures over two decades.
The landscape of cancer screening is a dynamic one, influenced by a confluence of factors including public health campaigns, accessibility of services, demographic shifts, and evolving medical guidelines. In Belgium, the participation rates in mammography screening for women aged 50 to 69 have been a subject of ongoing observation. From 1997, the percentage of women within this age bracket who reported having undergone a mammogram in the preceding two years demonstrated a consistent increase. This trend can be attributed to several key drivers. Enhanced public health initiatives across the European Union, including Belgium, have consistently advocated for regular cancer screenings, particularly for common malignancies like breast cancer, which disproportionately affect women in post-menopausal years. Furthermore, advancements in imaging technology have made mammography procedures more efficient and less uncomfortable, potentially reducing patient apprehension. The establishment and expansion of national or regional screening programs, often offering free or subsidized services, have also played a pivotal role in boosting uptake.
However, the reported dip in screening prevalence in 2018 warrants closer examination. While the overall trend has been positive, year-on-year fluctuations are not uncommon in public health statistics. Potential explanations for such a marginal decline could include temporary disruptions in service delivery, such as those experienced during unforeseen events, or shifts in survey methodologies. It’s also possible that the saturation point for screening has been reached within certain segments of the population, or that minor changes in recall periods within screening programs could influence the reported figures. International comparisons offer valuable context. Many developed nations have similar national screening programs for breast cancer, targeting women in the 50-69 age group. Rates of participation can vary significantly, influenced by healthcare system structures, cultural attitudes towards health, and the intensity of targeted public health campaigns. For instance, countries with highly centralized and actively managed screening programs often exhibit higher and more stable participation rates compared to those with more decentralized or opt-in systems.
The economic implications of mammography screening are multifaceted. On one hand, the direct costs associated with running screening programs – including equipment, personnel, and administrative overheads – represent a significant public health expenditure. However, these costs are often offset by substantial long-term savings. Early detection of breast cancer through mammography can lead to less aggressive and less costly treatments. Cancers identified at Stage 0 or Stage I are generally more treatable, often requiring less invasive surgery, fewer rounds of chemotherapy or radiation, and shorter recovery periods. This not only reduces direct medical expenses but also minimizes the indirect economic burden associated with lost productivity due to illness and extended recovery times. A healthier population is a more productive population, contributing to a stronger national economy. Moreover, the psychological and social benefits of early detection, including reduced patient anxiety and improved quality of life, are invaluable, though difficult to quantify in purely economic terms.
The survey data, which relied on a sample size of 1,569 respondents in 2018 for the specific age group and a broader sample for previous years, provides a snapshot of screening behavior. The methodology, involving an online survey, is a common approach for gathering such data, though it’s important to acknowledge potential biases inherent in online participation. The supplementary notes indicate that the figures are derived from statistical regressions, accounting for age, gender, and the Belgian population in 2018. This sophisticated statistical approach aims to extrapolate findings from the surveyed sample to the broader population, enhancing the reliability of the reported prevalence rates.
Looking ahead, maintaining and potentially increasing mammography screening rates will likely require continued investment in public health education, ensuring equitable access to screening facilities across all regions of Belgium, and potentially exploring innovative outreach strategies. As the population ages globally, the importance of effective cancer screening programs will only grow. Belgium’s experience, with its steady growth in screening participation over two decades punctuated by a minor recent dip, serves as a case study in the ongoing efforts to combat breast cancer through early detection and preventative healthcare. The long-term success of such programs hinges on sustained commitment, adaptive strategies, and a deep understanding of the factors influencing public engagement with essential health services.